
Last year, many raised concerns over the impact of prolonged lockdowns on children and young adults — kids who might lose large parts of their lives to a lockdown state as well as older adolescents, many of whom have missed out on pivotal rites of passage. Even more, losing their progress, their education, as well as their social and development to eight-hour “schooldays” spent on their devices – that is, if they are fortunate enough to have access to them and a stable home internet connection. Many are altogether losing out on an education, and what might perhaps be their only support system.
Concerns about adolescent suicide rates in the new normal of lockdowns have been met with assertions that the reverse was true. Warnings were dismissed, including reporting by the New York Times raising the question of hundreds of thousands of children not showing up to their online classes, lost to something or somewhere unknown. Little is known whether those children would return when in-person education returned. Even less known is in what state those children would return.
Even now, the available data on what happened in 2020, and is likely to continue into 2021, is sparse. The CDC’s systems are difficult to maneuver, for what data they might have, and are even now still working on incomplete data feeds from states. Information from individual states is even more disparate, with many still showing no health information or data more recent than January 2020.
In many ways, it is as if time stopped when 2020 began. For many, I am sure it still feels that way.
But now, we can slowly begin to look at what data is available and begin to piece together what happened and continues even now in many areas of America. This is a grim accounting for the lives of our children, the lives of young adults and teens, who were sacrificed on the altar of hesitant, improvised and chaotic pandemic policies. This is the cost of acquiescence to lobbying groups and propaganda of all types, and following “the science” blindly – when even then, those who were trying to do so were unable to accurately determine what would work, and what wouldn’t.
The course of the day was always absolute and beyond any dispute, even if yesterday’s wisdom said differently, and tomorrow’s would do likewise. Once the richly signaled morality crept into all pandemic responses in the US, there never was any room for nuance, for humility, or for balancing out the many other public health concerns. As we know, with the deferment of cancer screenings, treatments, and elective procedures, we have sacrificed far more than our kids on this altar.
But it is the kids who, unlike us adults, never had a say or voice in all this.
So, with what little information we have, what do we know?
In June, the CDC’s Morbidity and Mortality Weekly Report (MMWR) published data on emergency department (ED) visits for suicide attempts. This paints a grim picture, with a 51 percent increase in suicide attempts by teenage girls. What is less known is that very little was discussed about these numbers until the Surgeon General’s warning on the teenage suicide attempts came out in October. Media coverage of this report was a blip in June and resurfaced briefly in October. Even, so it has taken a few more weeks for coverage and segments, such as this last weekend’s Face the Nation, where there was finally an honest discussion on what this data might mean.
We also know from the Vital Statistics Rapid Release in August that there has been a very significant increase in overall opioid deaths in almost every state of the union. This data, though briefly written on, never seemed to catch hold in the broader public health discussion, but this is also beginning to change. There is a very slow momentum to recognize these reports, to understand what this data means, and what other data is currently not reported regarding 2020 and non-COVID public health-related issues.
Queries against CDC’s WONDER, their database and query system for overall public health data, reveal at least some of the measures of the close-to-complete data from 2020. Among these metrics are the underlying causes of death, as listed by the causes of death recorded on death certificates. By looking at this data, we can get an idea of non-disease-related fatalities, and to some extent, can at least speculate as to what and why we see the sometimes very stark changes and trends from 2018 to 2020.
Looking specifically at data on external causes of morbidity and mortality, there are relatively consistent numbers between 2018-2019 on a national scale, followed by drastic increases – often upwards of 20 percent (39.3k deaths in 2019 versus 48.5k deaths in 2020 for 25- to 34-year-olds).
It is important to understand the scale of changes. Overall, any individual metric might deal with hundreds, or maybe thousands of deaths total. Conversely, some of the percentages of increase are incredible, up to 179 percent even, for one specific age group and cause of death. These might be small numbers in absolute terms, but the spikes in what were previously stable (even if slowly increasing) trends are troubling. More so, they indicate that we have failed these people, these kids, and these areas of public health. Many of the starkest changes are among children, adolescents, and young adults. In the words of the great physiologist Harvey Cushing, who used the term to refer to young people dying from the Spanish Flu in the prime of their lives, these people are “doubly dead” – they never got to live.
In 2020, it was frequently stated that the overall suicide rate was down – true, over all age groups. The total number of suicides has gone down. For the 15-24 age range, the suicide rate increased by almost two percent, for the 24-34 age range by five percent, but the change for children between 5-14 years of age was twice as much – 10%.
Suicides are not at all the only measure that should be investigated. Many accidents are coded as such because they are unable to be coded as suicides, homicides, etc. Add to this that more children, teenagers, and young adults were put in positions where they were home alone, home with working parents, or home with minimal supervision. Some, not having in-person school, daycare, or normal amounts of time with adults present could easily get into things at home or engage in risky behavior, that they otherwise would not be able to do. It makes sense that with these kinds of factors there might be an increase in overall accidents for the 5-24 age groups in 2020 – and indeed, the data bears this out.
Transport accidents, though people drove less in 2020, actually increased across multiple age groups. For the 15-24 age range, transport fatalities increased by approximately 15 percent. Non-transport-related accidents, a broad catch-all category, increased by almost five percent for the 5-14 age range and a shocking 44 percent for 14–25-year-olds. Deaths from intentional discharges of firearms increased by 30 percent for ages 5-14 and by 13 percent for ages 15-24.
Deaths from drug overdoses increased across most age cohorts, but children, adolescents, and young adults were particularly hard hit. Eighty percent more children in the 5-14 age range died of drug overdoses in 2020 than in the previous year, while the number of deaths from drug overdoses in the 15-24 age group increased by 47 percent. Included in this are unintentional drug-related deaths – where we see 19 deaths in 2019 for ages 5-14 spiking to 52 deaths in 2020.
That might not seem like a lot in absolute terms, but the stunning increase of 179 percent in one year witnesses a barely occurring phenomenon becoming alarmingly more frequent. For other age groups, the figures are also significant: unintentional drug deaths increased by 56 percent for the 15-24 age range, and nearly 35 percent for the 25–34 age range.
Another disturbing data spike is the rise in deaths from assaults (i.e. intentional interpersonal violence). All three age groups (5-14, 15-24, and 25-34) saw increases greater than 30 percent in deaths from assault. More children, adolescents and young adults are dying from assaults than did in the last pre-pandemic year, 2019 – and one can think of a range of horrible and sad possibilities for what might be behind this spike.
America’s youth is afflicted with an epidemic of anomic suicide. The upheavals of the pandemic have left many young people disoriented, scared, confused and lost. Risk-taking, drug abuse, and violence are emotional outlets of normal people in an abnormal world. And with how much the adults have gotten wrong, any moral authority of their elders is – justifiably – suspect, and gradually devoid of any sway. And this epidemic is no less lethal than any virus.
Of course, there are limitations to this data, just as there are limits to what we know about overall overdose deaths and their demographics in 2020. The Vital Statistics Rapid Release provides a good start. We see an average increase, over the whole of the United States, of 22.7 percent in drug overdose deaths – most of them likely to be caused by opioids. But this data is limited, and since many of the states’ reporting is still incomplete, the numbers are actually under-reported. Even then, we see states with horrifying increases, well above the national average. Opioid deaths increased by 45.2 percent in California in just one year, in Mississippi, by 57 percent.
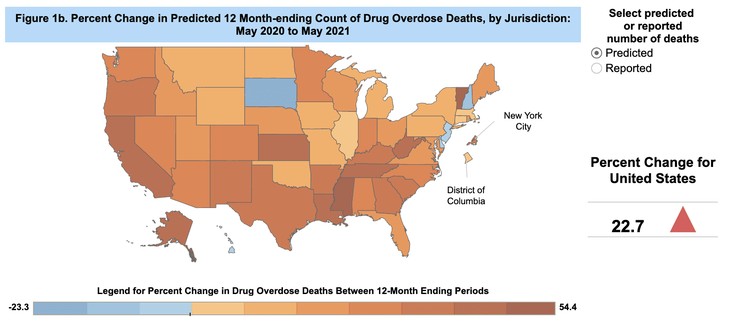
West Virginia, by 41.9 percent.
Kansas by 45.7 percent.
Alaska by 45.3 percent.
And Vermont by 54.4 percent.
It becomes difficult when we want to analyze this data, or the data in the CDC’s WONDER, any further. Vital statistics lag behind, and the pandemic has directed attention away from classical cause-of-death analyses. Much of the time, we would need to rely on state-level dashboards and data sets, which for many states, stop at 2019. For states that do provide more recent data, it might be limited, hard to obtain, difficult to access and analyze, or exist in a format that proves difficult for most data-driven epidemiologists to sift through.
For example, of the states with the highest increase in opioid overdoses, the next step would be looking at the demographic breakdown, to see year-on-year comparisons, who is being affected most and, maybe, come up with some theories as to why. Of the states listed above, only two provide much if any information that helps break down and compare the data in an accessible way.
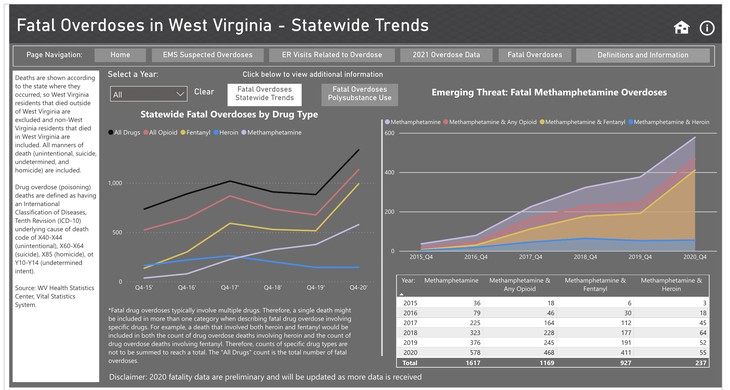
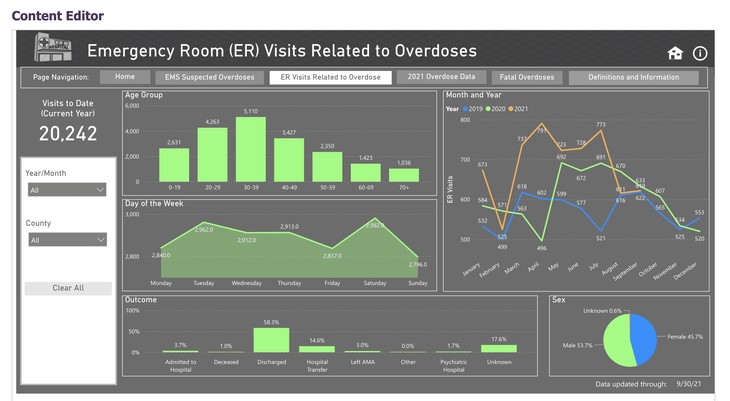
West Virginia has a simple dashboard, that shows some demographic breakdowns, ED visits, and deaths for drugs, with breakdowns as to the substances.
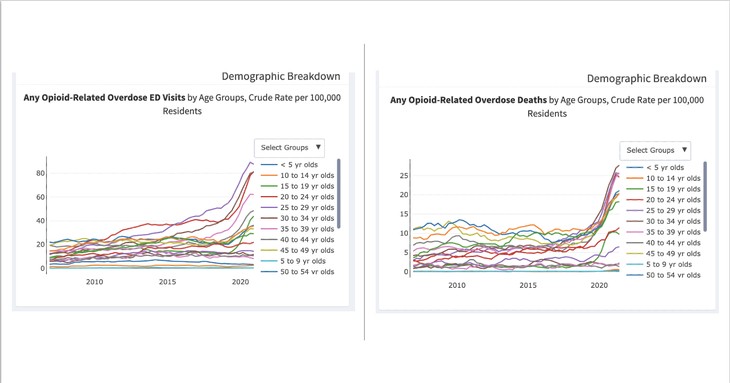
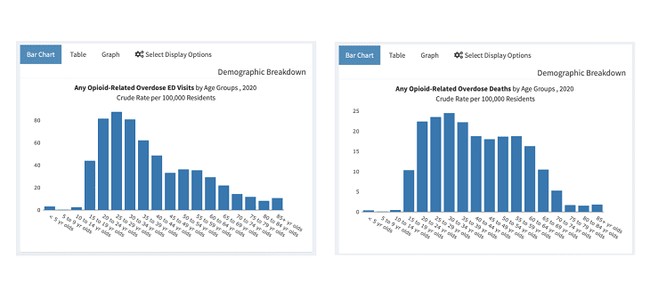
To give credit where it is due, the best available data and dashboard for this data set (from looking at the six states with the highest opioid death increases) comes from California, where one can compare and contrast years and demographics. What we can see from this data is a significant spike in ED visits and deaths related to opioids across many age groups between 2019-2020, including adolescents and young adults (please note in the screenshots, not all the age groups are visible in the color key).
Yet, without more available data from all the states, on all manners of death and hospital visits, digestible by demographics, a thorough understanding of what happened in 2020 remains elusive. What is clear, especially when compared to long-term (10-20 years) trends, is that 2020 caused many public health indicators to spike in a concerning manner, with many of these indicators impacting children and young adults at drastically different rates than older adults.
As we move into 2022, with no idea of when the full range of data from 2020 will be available (and even less so for 2021), it is important that we press for more data releases, better access, and a broader spectrum of public health indicators to be made publicly available – not only focusing on COVID, but also to understand and acknowledge the risks in which mitigation strategies have placed our most vulnerable. After nearly two years of explaining that everything we do is to save one life, one teacher, one grandparent, one child, there is really no longer any rationale to ignoring this data.
We’ve forever altered the trajectory of millions of young lives, and we owe it to them to not look away. To ignore neither the unfortunate and lasting impact, nor the doubly dead as Cushing called them, or the errors and egos that have led us here – so that we may one day at least recognize the errors. And perhaps, if we can manage, to apologize – by choosing not to ignore the silent and powerless at the behest of media or political alignment.
Owning up to this is long past due. We must understand how COVID-19 mitigation measures have impacted young people, through serious thought and study, rather than blindly fumbling in the dark as we did to get here – while also providing support, stability, and structure to those that we have deprived for far too long.











Join the conversation as a VIP Member